


Severe Mental Disorders and Stressful Life Events
[El trastorno mental grave y los sucesos vitales estresantes]
Karmele Salaberria1, 2, Alexander Muela1, 2, Maria Ruiz-Iriondo2, and Alvaro Iruin2
1University of Basque Country-Tolosa Hiribidea, San Sebastián, Gipuzkoa, Spain; 2Mental Health and Psychiatric Assistance, Neuroscience Department, Biogipuzkoa-Biodonostia Health Research Institute, San Sebastián, Gipuzkoa, Spain
https://doi.org/10.5093/clh2025a1
Received 8 March 2024, Accepted 16 July 2024
Abstract
Background: The relationship between stressful life events and development of severe mental disorders seems relevant. Method: The objectives were: to determine stressful life events in 166 patients with severe mental disorders; to compare levels of symptoms, internalized stigma, difficulties in emotional regulation and well-being between patients with and without a history of stressful life events; and to study the differential profile of patients according on gender. Results: The 75.3% mentioned a stressful life event that had significantly impacted their lives. Participants with a history of stressful events had poorer perceived health and more suicide attempts. They had less positive affect, greater intensity of psychopathological symptoms and difficulties in emotional regulation. From a gender perspective, bullying was the most reported stressful event among men, while sexual abuse was the most reported among women. Conclusions: It is necessary to assess and conduct long-term follow-up of children and adolescents to prevent theirs impact.
Resumen
Antecedentes: La relación entre sucesos vitales estresantes y la aparición de trastornos mentales graves parece importante. Método: Los objetivos del estudio fueron: determinar sucesos vitales estresantes en 166 pacientes con trastorno mental grave; comparar el grado de sintomatología, estigma internalizado, dificultades de regulación emocional y bienestar mental entre pacientes con y sin historia de sucesos; y estudiar el perfil diferencial en función del género. Resultados: El 75,3% mencionó un suceso vital estresante que le había influido marcadamente en su vida, estos participantes tenían peor percepción de su salud, más intentos de suicidio, menos afecto positivo, mayor intensidad de síntomas y más dificultades en la regulación emocional. El acoso escolar era el suceso vital que más afectaba a los hombres y el abuso sexual a las mujeres. Conclusiones: Resulta necesario evaluar y hacer un seguimiento a largo plazo de niños y adolescentes que hayan sufrido sucesos vitales estresantes para evitar sus efectos.
Palabras clave
Trastorno mental grave, Sucesos vitales estresantes, Conducta suicidaKeywords
Severe mental disorders, Stressful life events, Suicidal behaviourCite this article as: Salaberria, K., Muela, A., Ruiz-Iriondo, M., & Iruin, A. (2025). Severe Mental Disorders and Stressful Life Events. Clinical and Health, 36(1), 1 - 7. https://doi.org/10.5093/clh2025a1
Correspondence: mcarmen.salaberria@ehu.eus (K. Salaberria).The relationship between adverse or stressful life events and the development of severe mental disorders has been examined in various studies (Alvarez et al., 2011; Morgan & Gayer-Anderson, 2016; Petrucelli et al., 2019). Thus, experiences such as physical and sexual abuse, bullying, having witnessed maltreatment at home, or parents’ death in childhood have been associated with an increased risk of suffering severe mental disorders (Mansueto & Faravelli, 2021). The data underscore the impact of adverse events and psychosocial stress on mental well-being. Adverse, stressful, and traumatic life events are highly prevalent among the population with severe mental disorders compared to the general population (Grubaugh et al., 2011). Psychosocial stressors may play a crucial role in the onset of psychosis, increasing the likelihood of its occurrence (Shevlin, et al. 2007). Bentall et al. (2012) found that sexual abuse in childhood is related to the onset of auditory hallucinations in adulthood and that having suffered bullying is related to the onset of paranoid ideation. In many cases, it is difficult to distinguish between the symptoms of post-traumatic stress disorder (PTSD) and the symptoms of psychosis (Compean & Hamner, 2019). Childhood adverse life events have also been associated with an increased risk of substance abuse, suicidal ideation and attempts, and psychotic experiences (Sachs-Ericksson et al., 2016; Setién-Suero et al., 2020; Varese et al., 2012). Specifically, in patients with schizophrenia, traumatic events in childhood are associated with an increased risk of suicide, a worse response to treatment, and poorer social functioning (Li et al., 2015). Thus, there are high rates of suicidal ideation and behavior among patients with severe mental disorders who have suffered adverse events (Grubaugh et al. 2011). Besides, adverse events in childhood and adolescence contribute to poorer cognitive and social functioning and are a risk factor for developing severe mental disorders (Mayo et al., 2017). A history of victimization and adverse early life experiences produce physical and psychological vulnerability and an increased inability to cope with everyday stressful events (Hardy, 2017). All these variables, along with negative beliefs about one’s mental illness and the stigma associated with the disorder, are related to a lower level of mental well-being and more emotion-regulation difficulties (Khoury & Lecomte, 2012; Ropaj et al., 2021). The latter appears to be an important mediating factor between adverse experiences and the development of psychotic symptoms (Lincoln et al. 2017). From a gender difference perspective, it has been found that in patients with psychosis men have experienced more physical abuse and women have suffered more sexual abuse compared to controls from the general population (Mansueto & Faravelli, 2021). However, despite these data, few studies have been conducted in Spain evaluating the presence of adverse life events in patients with severe mental disorders and the differential profile of men and women. The objectives of this study are: a) to determine the presence of adverse life events in a sample of patients with a chronic severe mental disorder; b) to compare the levels of symptomatology, internalized stigma, difficulties in emotion regulation, and mental well-being, between patients with and without a history of adverse events; and (c) to study the differential profile of patients according on gender. Related to the study’s objectives, the following hypothesis are presented: a) more than half of the patients with severe mental disorders will have experienced significant stressful life events; b) patients with stressful life events will exhibit more psychopathological symptoms, lower positive affect, and greater emotional interference; and c) men will identify physical abuse as more important adverse life events, while women will identify sexual abuse. A descriptive and cross-sectional design was used to describe a convenience sample of patients with a severe mental disorder and a two-group comparative design was used to analyze the differences between patients with and without adverse life events. Participants The inclusion criteria were: a) suffering from a severe mental disorder, such as a schizophrenia spectrum disorder, a mood disorder (i.e., bipolar disorder, chronic depression) or a personality disorder; b) being over 18 years of age; c) being able to complete the assessment instruments; d) being clinically stable and complying with medical guidelines; and e) providing consent to participate in the study. The participants were 166 patients with a severe mental disorder who regularly attended the following centers or day hospitals: Gipuzkoan Association of Relatives and People with Mental Illness (AGIFES), Biscayan Association of Relatives and People with Mental Illness (AVIFES), Alava Association of Relatives and People with Mental Illness (ASAFES), Ayalesa Association of Relatives and People with Mental Illness (ASASAM), and AITA MENNI Day Hospitals in Beasain, Donostia, Irún, and Arrasate. The participants had a mean age of 50 years, 105 being men, and 61 were women. Most were single, and their level of education was mainly secondary and most had an income between €500 and 1,000 (see Table 1). Concerning mental health, 77% were diagnosed with schizophrenia, 12.7% with bipolar disorder, 8.4% with personality disorder, and 1.8% with depressive disorders. The average time elapsed since diagnosis was 21 years; thus, the participants presented chronic problems. Table 1 Sociodemographic Data 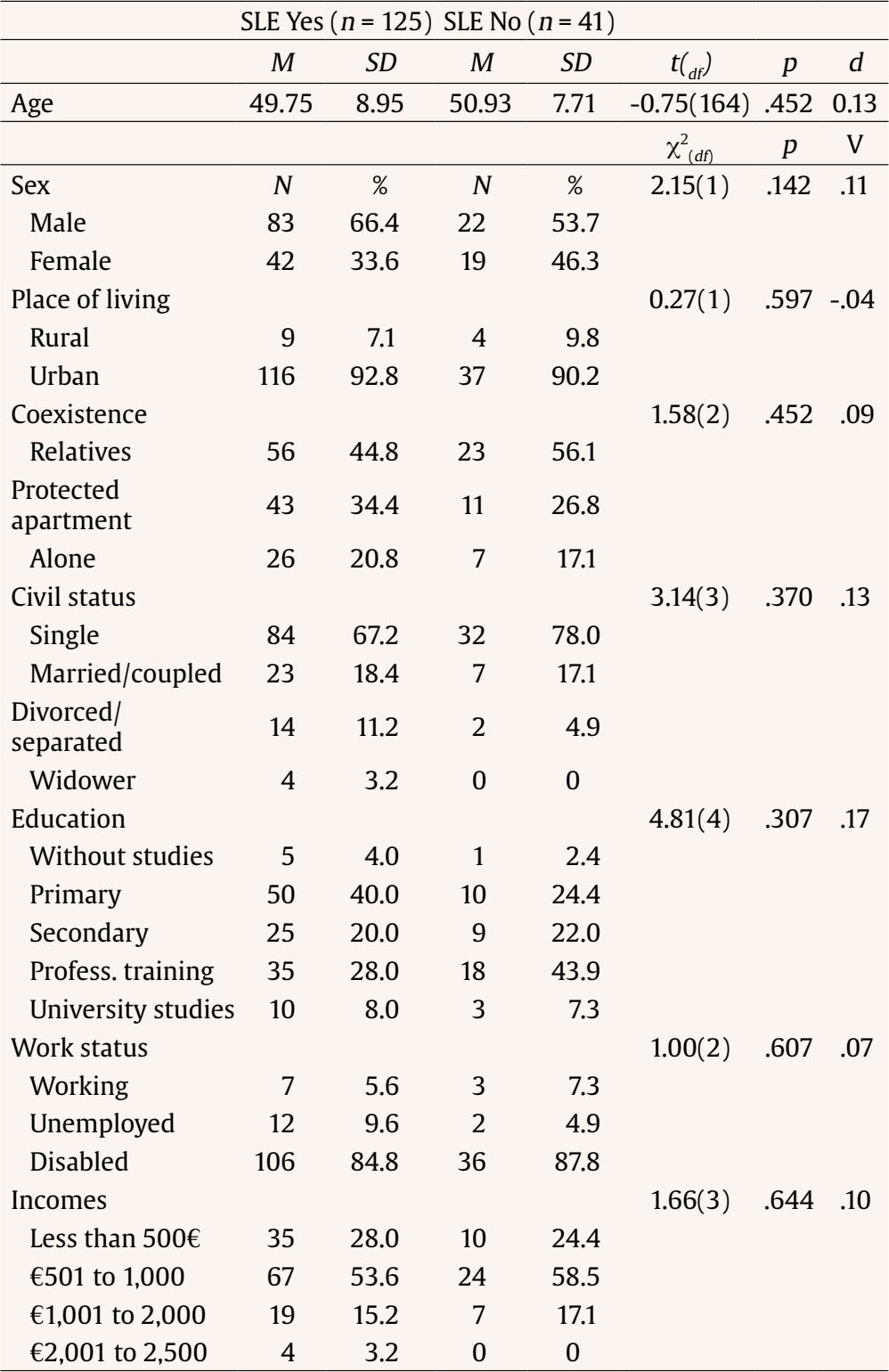 Note. SLE = stressful life events. Procedure The study was conducted at the patients’ day centers in 2019 and 2021. During 2020 no personal interviews were carried out due to COVID-19. All procedures contributing to this study were performed following the Helsinki Declaration of 1975, revised in 2008, and were approved by the Ethics Committee of the Department of Health of the Basque Government (CEIm-E) (PI2019003). Participants were assessed face to face by a general health psychologist (the third author) after being informed of the study’s objectives and giving informed consent to participate. Consenting participants were individually assessed in two 1-hour sessions. Measures Demographic and Health Variables Each participant was interviewed and asked to provide information about several demographic and health variables, including age, sex, civil status, work status, substance abuse, diagnosis, number of psychiatric admissions, suicide attempts, and self-perceived health. Adverse or Stressful Life Events The first section of the Global Post-Traumatic Stress Assessment Scale (EGEP; Crespo-Gómez, 2012) was used to evaluate the presence of stressful life events. This section comprises a list of 12 events. The patient responds whether any of these events has happened to him/her and at what age. After indicating the events, patients are requested to choose the one that has caused or causes the most discomfort. This event was used to carry out the analyses of the study. The scale presents good internal consistency with an α = .90. Table 2 Health Related Variables 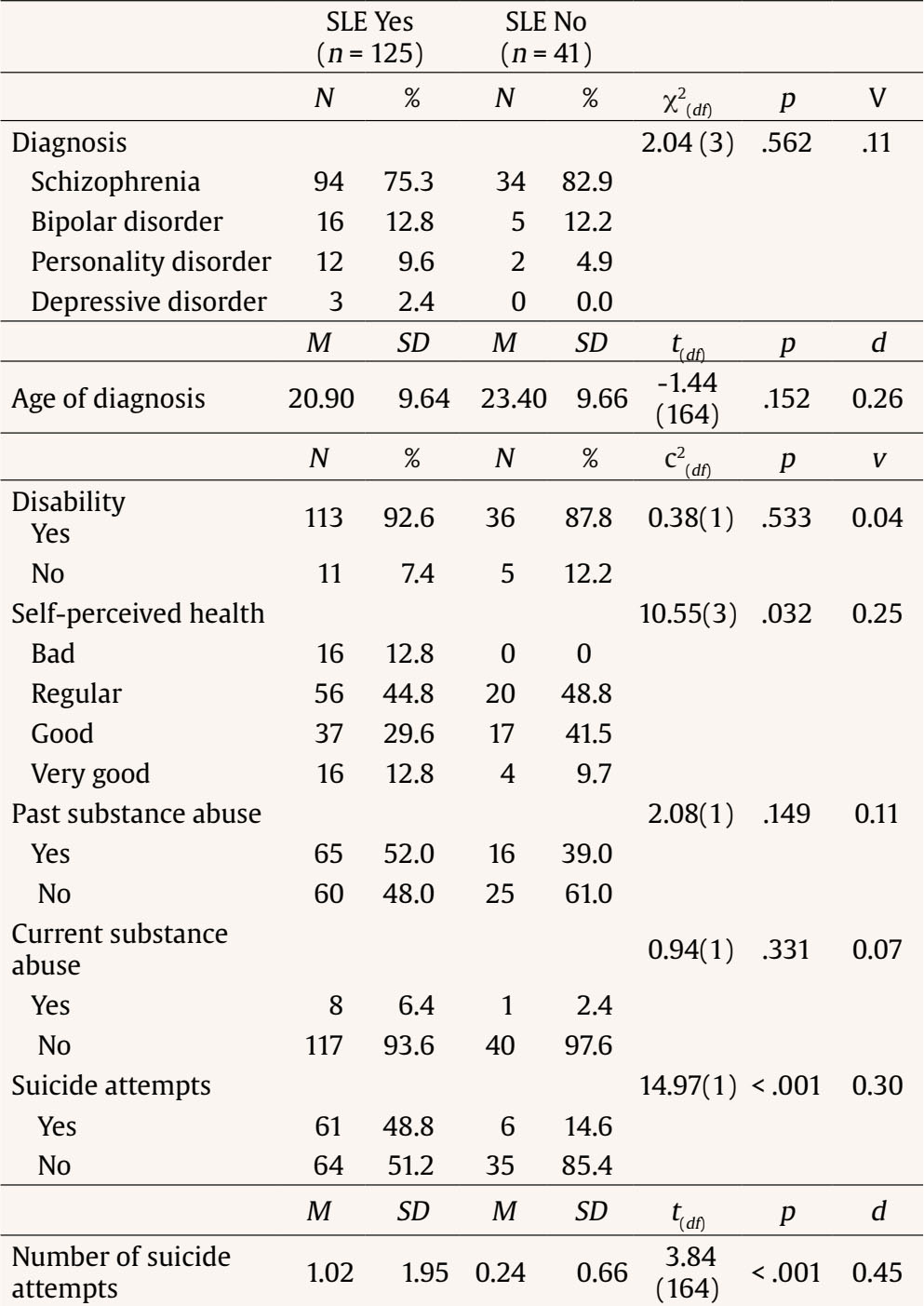 Note. SLE = stressful life events. Psychopathological Symptoms, Stigma, and Emotion-regulation Difficulties PANAS Scale of Positive and Negative Affect (Watson et al., 1988; Spanish version by Sandín et al., 1999). This 20-item questionnaire is divided into two subscales of 10 items each: Positive Affect and Negative Affect. Items are rated on a 5-point Likert scale ranging from 1 (not at all) to 5 (a lot) (range = 10-50). A higher score indicates greater positive and negative affect. The α reliability of the Positive Affect subscale ranges from .87 to .89, and the α of the Negative Affect scale ranges from .89 to .91. Brief Symptom Checklist (LSB-50; De Rivera & Abuin, 2012). This instrument comprises nine clinical scales (psychoreactivity, hypersensitivity, obsession-compulsion, anxiety, hostility, somatization, depression, sleep disturbance, and expanded sleep disturbance), a psychopathological risk index, three global indices (frequency of symptoms, intensity, and global impact), and two validity scales (minimization and magnification). Items are rated on a 5-point Likert scale ranging from 0 (not at all) to 5 (a lot). Higher scores indicate high levels of psychopathological distress, coefficients α ranging from .79 to .90. Table 3 Psychopathology, Social Support and Well-being  Note. SLE = stressful life events. Table 4 Internalized Stigma and Emotional Regulation 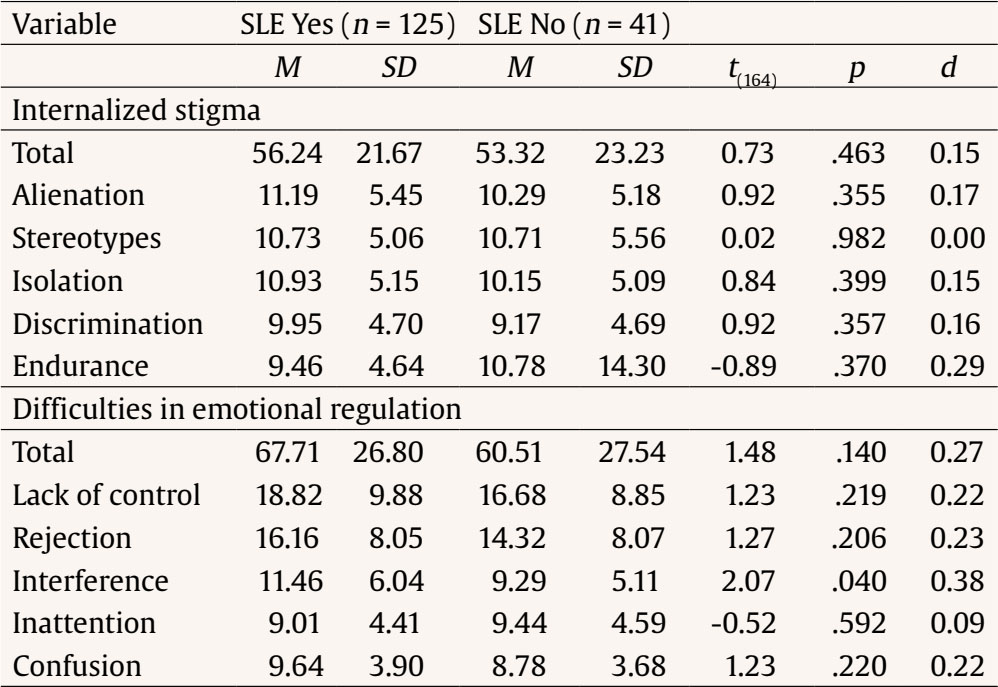 Note. SLE = stressful life events. The Mental Illness Self-Stigma Scale (ISMI; Boyd et al., 2003; Spanish version by Bengoechea-Seco et al., 2018). This self-report assesses the subjective experience of stigma. It consists of 29 items divided into several subscales: Alienation (6 items), Stereotyping (7 items), Discrimination (5 items), Social Isolation (6 items), and Resistance to Stigma (5 items). All subscales are scored on a 4-point Likert scale ranging from 1 (strongly disagree) to 4 (strongly agree). The first four subscales are scored directly and the last scale is scored inversely. The total score and scores obtained in the subscales can be divided by the number of items to compare results with the Spanish version. Higher scores indicate high levels of self-stigma. The instrument shows good psychometric properties, with an internal consistency of .91 and a reliability of .95. The Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, 2004: Spanish version by Hervás & Jódar, 2008). This 28-item scale explores different aspects of emotion regulation. Thus, the scale evaluates emotional lack of control (9 items), emotional rejection or non-acceptance of discomfort (7 items), daily interference such as difficulties in concentration and task performance (4 items), difficulties in attending to and knowing one’s emotions (4 items), and emotional confusion (4 items). Each item is scored on a 5-point Likert scale ranging from 1 (almost never) to 5 (almost always), the range of total score being 28-140. The higher the score, the more the difficulties in regulating emotions. The instrument shows good internal consistency, between .73 and .71, and good test-retest reliability, .74. Table 5 Type of Event and Differences between Men (n = 83) and Women 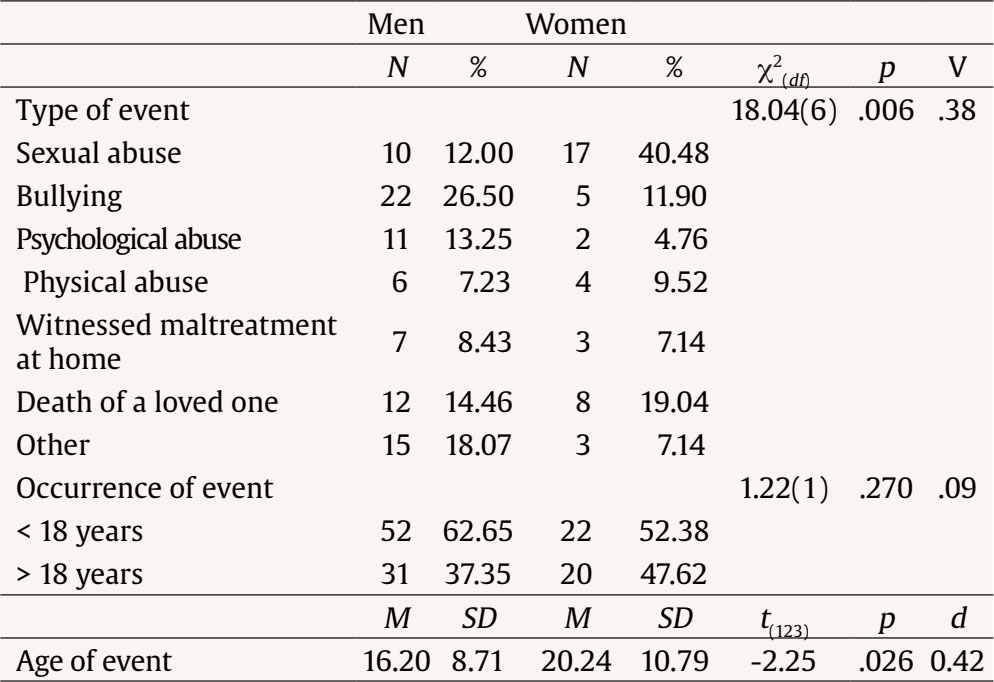 Mental Well-being Warwick-Edinburgh Mental Well-being Scale (WEMWBS; Tennant et al., 2007; Spanish version by Andrée-López et al., 2013). This 14-item scale assesses a patient’s feelings and thoughts about mental well-being. It is rated on a 5-point Likert scale ranging from 1 (never) to 5 (always). Global score is obtained adding all the items (range 14-70), higher scores indicating higher levels of mental well-being. The instrument has good internal consistency, .89-.91, and good test-retest reliability, .83. Data Analysis The G*Power program was used to calculate the sample size, estimating an effect size of 0.5, a probability of error of .05, and a beta of .80, resulting in the need for a sample of 128 participants. Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS v.26). Data were first explored with descriptive statistics: means and standard deviations for quantitative variables and frequencies and percentages for qualitative variables. Group differences were analyzed using a chi-square test for categorical variables, and Student’s t test for independent measures. Kramer’s V and Cohen’s d were calculated to estimate the magnitude of the differences between the groups. Considering stressful life events, of the 166 participants, 125 (75.3%) mentioned some adverse event that had significantly impacted their lives. Of these patients, 21.6% reported sexual abuse and bullying, respectively, 10.4% reported psychological abuse, 8% physical abuse, 8% witnessed maltreatment at home, 16% bereavement, and 14.4% mentioned another type of stressful event. The mean age of occurrence of the stressful event was 17.56 years (SD = 9.6) with a range between 4 and 40 years. Additionally, 59.2% indicated that the event had occurred before the age of 18 and 40.8% afterward. Differences between Patients with and without Stressful Life Events We compared the patients who reported adverse events that significantly impacted them and the patients who did not report such events in the target variables. Considering the sociodemographic aspects, there were no significant group differences (see Table 1). Concerning health, patients with adverse events had worse perceived health, with a small difference effect size, and had made more suicide attempts compared to patients without adverse life events, with a large difference (see Table 2). Patients with severe mental disorders who reported adverse life events presented a higher proportion of suicide attempts, 48.8% versus 14.6%. Table 3 shows group differences in the psychopathological and mental well-being variables. Thus, patients who had suffered adverse events had less positive affect, more intense psychopathological symptoms, and higher scores in sleep difficulties, with moderate size differences. They also perceived less mental well-being, although the difference was not statistically significant. Concerning internalized stigma (see Table 4), people who reported adverse life events had higher scores on both the total scale and the different subscales, although without statistically significant differences. Likewise, they presented more emotion-regulation difficulties (see Table 4), with significant differences in the interference produced, which can lead to difficulties in concentration and task performance. The scores of the study participants were above the cut-off points used in the Spanish validation of the instrument (Hervás & Jódar, 2008). Patients with Stressful Life Events: Gender Differences The differential profiles according to the sex of the 125 patients who reported an adverse life event are analyzed. The most adverse events reported by the participants were sexual abuse in the case of women (40.48%) and being a victim of bullying in the case of men (26.5%). They are followed by traumatic grief, usually associated with parents’ death, and being a victim of abuse. In the Other category, patients mentioned romantic breakups, work problems, childhood with parents’ traumatic separations, and involuntary psychiatric admissions. The mean age of occurrence of the events was adolescence in men and early youth in women, and this difference was statistically significant (see Table 5). A comparative analysis was performed between men with and without adverse life events and women with and without adverse events in all the variables evaluated in the study. Table 6 shows only statistically significant comparisons. Table 6 Significant Differences between Men with and Without SLE and between Women with and without SLE 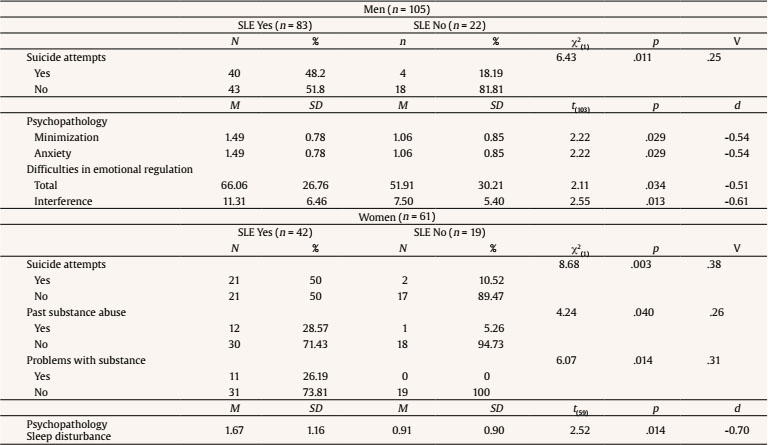 Note. SLE = stressful life events. Among the 105 men with a severe mental disorder, 79.04% had a history of traumatic events compared to 20.95% who had no such history. Differences between the two groups were observed in the presence of suicide attempts, which was much higher among men with a severe mental disorder and a history of adverse events. In addition, these men presented greater minimization of symptoms and more anxiety. They presented more emotion-regulation difficulties and interference from emotions. The differences in these variables were moderate. In the case of women, of the 61 women with a severe mental disorder, 68.85% had a history of victimization compared to 31.14% who did not. Women with a history of victimization had made more suicide attempts, presented more problematic substance use, and had more sleep disturbances, and these differences were moderate to large in size. From the data obtained, it can be observed that 75% of the participants in the study presented adverse life events that had significantly impacted their lives, which confirms the study’s hypothesis. This proportion is higher than the general population’s (Comacchio et al., 2019). In Spain, approximately 9% of men and 22% of women report having experienced sexual abuse (Pineda et al., 2023) and 24.6% of students having suffered from bullying (Fundación ANAR & Mutua Madrileña, 2023). In a recent study with young people from the general population aged between 12 and 25 years old, 53.44% reported having experienced an adverse life event (Marrero et al., 2024). In both men and women participants, more than half of the sample indicated that these events occurred before the age of 18, which shows the importance and impact of stressful life events occurring in childhood and adolescence in the development of severe mental disorders (Stevens et al., 2017). Men indicated an average of 16 years and women an average of 20 years as the age where stressful events impacted the most. Perhaps a relationship could be established between the occurrence of these events and the age of the first psychotic episode, which typically occurs between 18 and 19 years in men and between 20-25 years in women (Solmi et al., 2021). From a comparative point of view, in this study patients with severe mental disorders and a history of stressful life events have worse perceived health, less positive affect, more sleep problems, perceive more interference of emotions, and have made more suicide attempts. Their profile is more severe and the history of victimization makes these people a particularly vulnerable group. Similar results were found in the study of Fontanil et al. (2021), therefore the study’s second hypothesis is fulfilled. Participants with a severe mental disorder and a history of adverse life events make more suicide attempts than patients without such a history. In the study by Mohammadzadeh et al. (2019) being a victim of sexual abuse was a predictor of suicide attempts in hospitalized patients with schizophrenia, and in the meta-analysis of Ng et al. (2018) it was a variable that increased suicide risk. In this study, comparing men with and without stressful life events the former had more anxiety and difficulties with emotional regulation and women with stressful life events had a problematic history of substance use. Similar results were also found by Lopez-Diaz et al. (2018), Setién-Suero et al. (2020), and Tomassi et al. (2017). Considering the type of life event that had affected them most, the profile between men and women differs. In both cases, grief or loss of loved ones are mentioned, but in the case of men being victims of bullying and in the case of women sexual abuse appear as more impacting events. These results are similar to those of Comacchio et al. (2019), Mansueto and Faravelli (2020), Misiak et al. (2016), and Misra et al. (2019). In the case of men with stressful life events, bullying emerges as the most impacting event. This result is similar to the review by Mayo et al. (2017), where bullying was associated with poor self-esteem, depression, suicidal behavior, and risk of psychosis. Being a victim of bullying can facilitate the development of negative cognitive schemas of external locus of control and increase symptoms like suspicion and paranoia (Gibson et al., 2016). In the case of women, sexual abuse was the most frequently mentioned event. In the study by Bourgeois et al. (2021) sexual abuse was identified as one the most significant factors contributing to the development of psychotic disorders, particularly when accompanied by substance abuse. The results of this study point to the need to evaluate the history of adverse life events in the population with severe mental disorders and to offer treatment for these patients. Studies of people with PTSD usually exclude people with psychosis for fear of exacerbating the symptoms or provoking a relapse. Thus, in the few studies of samples with comorbidity, psychoeducation on PTSD, breathing training, and cognitive restructuring have been used with encouraging results (Mueser et al., 2008). Exposure, a central element in treating post-traumatic stress, has been less studied in samples with a severe mental disorder. This study has some limitations, such as the type of retrospective evaluation carried out, which may affect the reliability of the data. Besides, some patients were evaluated after the COVID period when day centers were reopened; perhaps during this period symptoms may have worsened. It would have been of interest to have a control group without severe mental disorders but with stressful life events to enable comparisons. Furthermore, it was also impossible to register the age at which the suicide attempt or attempts were made. Increasing the sample size would allow more powerful analyses and longitudinal follow-ups of patients so that the course of psychopathology could be assessed. We could better understand the concatenation of psychological difficulties, including substance abuse, onset of the severe mental disorder, and to know when suicide attempts occur. Some implications for clinical practice and prevention are derived from this study’s results. It is necessary to systematically evaluate the presence of adverse life events in the child and adolescent population. Long-term follow-ups of those who have experienced bullying and sexual abuse or the loss of loved ones in childhood are necessary because of the impact of these events and their possible causal relationship with the development of severe mental disorders (Merrick, 2019). Finally, special attention should be paid to the impact of a history of adverse or stressful life events on the onset of substance use and suicide risk. It is essential to provide coping strategies to the victims of adverse life events to relieve their distress and promote recovery. Highlights
Conflict of Interest The authors of this article declare no conflict of interest. Acknowledgements We appreciate the collaboration of the AGIFES, AVIFES, ASAFES, ASASAM, and AITA MENNI. Cite this article as: Salaberria, K., Muela, A., Ruiz-Iriondo, M., Iruin, A. (2025). Severe mental disorders and stressful life events. Clinical and Health, 36(1), 1-7. https://doi.org/10.5093/clh2025a1 Funding Bottom-up 17BU-101 & 20BU-102 projects. Departament of Health of the Basque Government. References |
Cite this article as: Salaberria, K., Muela, A., Ruiz-Iriondo, M., & Iruin, A. (2025). Severe Mental Disorders and Stressful Life Events. Clinical and Health, 36(1), 1 - 7. https://doi.org/10.5093/clh2025a1
Correspondence: mcarmen.salaberria@ehu.eus (K. Salaberria).Copyright © 2025. Colegio Oficial de la Psicología de Madrid






 PDF
PDF e-PUB
e-PUB CrossRef
CrossRef JATS
JATS Print
Print Send
SendEMAIL ALERT
Clinical and Health is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License








